Welcome to the CJU website »
LOG IN

 Indexed in Index Medicus and Medline
Indexed in Index Medicus and Medline
HOW I DO IT
Novel knot tying technique for robot-assisted surgery
Khurshid A. Guru, MD,1 Mohd Raashid Sheikh, MD,1 Syed J. Raza, FCPS,1 Andrew P. Stegemann, BS,1 John Nyquist, MS2
1Department of Urology, Roswell Park Cancer Institute, Buffalo, New York, USA
2Department of Pathology and Anatomical Sciences, State University of New York, Buffalo, New York USA
GURU KA, SHEIKH MR, RAZA SJ, STEGEMANN AP,
NYQUIST J. Novel knot tying technique for robot-assisted surgery. Can J Urol 2012;19(4):6401-6403.
Robot-assisted surgery has seen significant advancements in recent years, with dedicated training opportunities to acquire adequate skills. With improved degree of rotation and movement offered by the robot arm, newer techniques of knot tying need to be developed. Here we present a novel method of knot tying to help place a secure knot, especially with short suture length.
Key Words: robotics, surgical technique, knot tying
The field of surgical sciences has evolved over the last decade with the evolution of a minimally invasive robot-assisted approach. The initial era of robot-assisted surgery witnessed the development of skills through self-learning and short term mentoring methods, however, dedicated and well-structured robotic surgery fellowships are now available.1 The importance of training and development is highlighted by the fact that in a survey of 297 surgeons, 78% felt that robot-assisted surgical training was required and given an opportunity, 83% would consider robot-assisted surgical training.2 Procurement of appropriate surgical skills is important, especially when considering that robot-assisted surgery provides a greater degree of instrument movement within the same confines when compared to laparoscopic surgery.
Knot tying is a fundamental surgical skill that must be performed efficiently, and has equal importance in robot-assisted surgery. Due to the added advantage of EndoWrist (Intuitive Surgical Inc., Sunnyvale, CA, USA) technology and three-dimensional vision, conventional knot tying methods may need some modification to suit the robotic surgical environment. We therefore developed a novel method for tying a knot, which can be particularly helpful for tying short length sutures. In addition to being a time efficient technique, it allows for secure knot placement to address the needs of minimally invasive surgery.
In this technique, the surgeon begins by grasping the right end (blue color thread) of the suture without touching the left end (black color thread), Figure 1a. The right end of suture is crossed over the left end to create a loop, Figure 1b. The right instrument is next passed under the loop, created by the crossing right end of suture, and grasps the crossed over right end, Figure 1c.
The right end is then pulled by the right instrument underneath the left suture, which is still untouched, Figure 1d. The left instrument grasps the left suture and the two ends are pulled apart to form the knot, Figure 1e and 1f. Another knot can be placed over it in an alternating but similar fashion without swapping arms.
Surgical knots are recognized as an important element of surgical performance and technique. Whether performed conventionally or robotically, the failure rate is variable and depends on the suture material, not the method of knot tying.3 Furthermore, knot tying can consume a substantial duration of the surgery.4 With the advent of advanced laparoscopic procedures, different novel techniques of knot tying have been devised.5,6 Limited instrument maneuverability, two-dimensional vision and a fulcrum and pivoting effect make it difficult to tie knots laparoscopically. A study of 22 participants who performed suturing tasks using laparoscopic robotic modules found the EndoWrist technology and three-dimensional vision of the robot to be
beneficial.7
Robot-assisted and laparoscopic surgery can be compromised by the use of short suture length in order to accommodate instrument movements within a restricted space. The primary value of this featured knot tying technique is in its efficiency for tying short length sutures. Shorter length sutures are frequently encountered during intracorporeal suturing in robot-assisted surgery. This technique allows the surgeon to use the three-dimensional vision and EndoWrist technology with 60 of freedom of movement of the da Vinci robot. These knots can be placed safely without exaggerated movements that could compromise tissue integrity or cause collision of the robotic arms. This may be advantageous with the continued evolution of single port surgery. The technique is less time consuming and therefore highlights the importance of efficiency in suturing during major intra-corporeal reconstructive procedures. In addition to the aforementioned benefits, this technique is easy to learn and implement. In the future we would like to determine the strength of this type of knot and further document its safety and efficacy.
We present a novel method of knot tying for robot-
assisted surgery. Further application in different fields of
robot-assisted surgery will help prove its efficiency.
Accepted for publication June 2012
Address correspondence to Dr. Khurshid A. Guru, Department of Urologic Oncology, Roswell Park Cancer Institute. Elm and Carlton Streets. Buffalo, New York 14263 USA
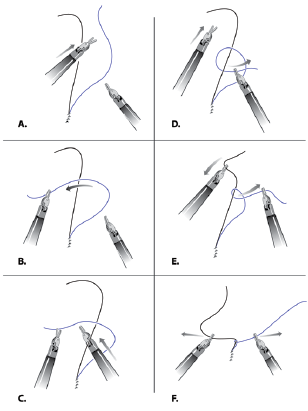
Figure 1a-1f. Key steps towards novel knot tying technique.
1. Schreuder HW, Wolswijk R, Zweemer RP, Schijven MP,
Verheijen RH. Training and learning robotic surgery, time for a more structured approach: a systematic review. BJOG 2012;
119(2):137-149.
2. Guru KA, Hussain A, Chandrasekhar R, Piacente P. Current status of robotic- assisted surgery in urology: a multi-national survey of 297 urologic surgeons. Can J Urol 2009;16(4):4736-4741.
3. Muffly T, McCormick TC, Dean J, Bonham A, Hill RF. An evaluation of knot integrity when tied robotically and conventionally. Am J Obstet Gynecol 2009;200(5):e18-e20.
4. Herrmann JB. Tensile strength and knot security of surgical suture materials. Am Surg 1971;37(4):209-217.
5. Soper NJ, Hunter JG. Suturing and knot tying in laparoscopy. Surg Clin N Am 1992;72(5):1139-1152.
6. Gopaldas RR, Reul RM. Intracorporeal knot-tying for the thoracoscopic surgeon: a novel and simplified technique.
Tex Heart Inst J 2010;37(4):435-438.
7. Guru KA, Kuvshinoff BW, Pavlov-Shapiro S, Mohler JL. Impact of robotics and laparoscopy on surgical skills: A comparative study. J Am Coll Surg 2006; 204(1):91-101.
Current Issue
December 2024, Vol.31 No.6