Indexed in Index Medicus and Medline
Indexed in Index Medicus and MedlineIntroduction
The burden of prostate cancer is tremendous, accounting for approximately 241,000 new cases and 34,000 deaths in the United States in 2011.1 Furthermore, prostate cancer is the second leading cause of cancer deaths in men behind only lung cancer.1 Despite the favorable stage migration seen since the advent of prostate-specific antigen (PSA) screening, extraprostatic disease continues to be detected in 38%-52% of patients undergoing radical prostatectomy (RP),2,3 and 5-year biochemical recurrence (BCR) rates after surgery remain between 15%-40%.4,5 In light of these pathologic data, radiation therapy (RT) after RP has been assessed in both the adjuvant and salvage settings.
Initial reports from two contemporary randomized trials of adjuvant RT versus observation both noted that adjuvant treatment provided improvements in BCR-free survival and clinical recurrence-free survival.6,7 Similarly, a separate recent study found that salvage RT was associated with a three-fold increase in prostate cancer-specific survival.8 These favorable trial results argue for the routine use of post-prostatectomy RT.
The goals of radiotherapy are to deliver a therapeutic amount of radiation to the intended target tissue while limiting toxicities to surrounding structures. The ability to localize the intended target is paramount in achieving these purposes. In patients being treated with primary RT for prostate cancer, prostate position has been shown to vary daily, and can be influenced by bladder and rectal volumes. Unfortunately, targeting the prostatic fossa after RP is especially difficult, as it is subject to motion and positioning errors due to the bony pelvic anatomy, bladder volumes, and rectal distension.
More recently, the placement of radiopaque fiducial markers and electromagnetic transponder beacons (Calypso Medical Technologies, Seattle, WA, USA) have been introduced as a method to improve prostate localization and make daily target adjustments during RT for prostate cancer. These techniques have been shown to be technically feasible and appear to improve the precision of treatment. However, the reports to date have largely been limited to patients undergoing primary RT, such that little data exist on the optimal method to target the prostate bed for post-RP RT.
For patients who require RT following RP limited data exist regarding the optimal method to achieve target localization. A single study reported placing gold seed fiducial markers into the prostatic bed of 10 patients who were undergoing adjuvant or salvage radiotherapy.9 The Calypso system relies on a wireless magnetic tracking system and is used for primary RT for prostate cancer. We recently reported our initial experience with the implantation of transponder beacons into the prostatic bed of patients after RP to aid in target localization for adjuvant and salvage RT. We noted no adverse events attributable to the procedure, including a post-procedure febrile illness, urinary retention, hematuria, or rectal bleeding.10 Furthermore, short and intermediate term side effects were mild, and short term oncologic results were encouraging.10 In this report, we detail our procedure and technique for implanting the electromagnetic transponders in patients undergoing radiation therapy after radical prostatectomy.
Methods
Placement of the electromagnetic transponders is an outpatient procedure performed under local anesthesia in the office setting. Any patient who is deemed a candidate for adjuvant or salvage radiation therapy after radical prostatectomy is suitable for this procedure. For the purpose of clarity, we define adjuvant therapy as radiation treatment delivered to patients after RP with an undetectable PSA but who have high-risk pathological features, such as positive surgical margins, extracapsular extension, or seminal vesicle invasion. Salvage therapy was defined as RT delivered to patients with a detectable and/or rising PSA after surgery.
Prior to proceeding with transrectal implantation, the patient should complete a consultation with a urologist and/or a radiation oncologist to describe the technique of transponder implantation as well as the process of post-RP radiation therapy. As part of the initial process, patients are evaluated with a magnetic resonance imaging (MRI) simulation of the prostate bed, whereby the patient is placed in a supine position and immobilized. A closed 1.5T MRI –simulator is used to acquire a non-contrast volumetric scan. The scan encompasses approximately 1 cm above the bladder to 1 cm below the penile bulb using 3 mm axial slice thickness with a T2-weighted 3-dimensional turbo spin-echo sequence. The MRI images are processed for image distortion correction using gradient distortion correction software. After this imaging study, the patient is now ready for Calypso beacon placement. As a final step at our institution prior to transponder placement, the patient will complete the American Urological Association Symptom Score (AUA-SS) and the Sexual Health Inventory for Men (SHIM) to assess for treatment toxicities as well as monitor for side effects during and after the completion of radiation therapy.
Preprocedure instructions
1) Anticoagulants and antiplatelet agents should be stopped at the appropriate time before the procedure, usually 7 days prior to implantation. Patients on warfarin will have an INR measured prior to proceeding with procedure. In patients with drug-eluding stents, the beacon implantation is performed on low dose aspirin. The patients are counseled regarding the risks of acute stent thrombosis when stopping anti-platelet agents versus the risks of performing transrectal prostate biopsies while continuing anti-platelet therapy with aspirin.
2) The patient is instructed to take all of his other regular medications as directed the morning of the procedure.
3) 1 gram of intramuscular (IM) Rocephin is administered prior to the procedure.
4) The morning of the office procedure an enema is given to empty the rectal vault so that the vesico-urethral anastomosis can be better visualized during transrectal ultrasound.
The procedure
1) The patient is placed in the left lateral decubitus position on the examining table. A generous amount of 2% lidocaine jelly is then inserted into the rectal vault to aid in achieving local anesthesia.
2) An adequately lubricated ultrasound probe is then placed into the rectum and the bladder and surrounding landmarks are identified.
3) Using the sagittal ultrasonographic views, the bladder and vesico-urethral anastomosis are imaged, Figures 1a and 1b.
4) Five cc of 1% lidocaine are administered to the left and right of the vesico-urethral anastomosis for local anesthesia.
5) Another 5 cc of 1% lidocaine is then injected anterior to the rectal wall to create separation between the urethra, vesico-urethral anastomosis, bladder, and rectum, Figures 1a, 1b, and 2. This injection is very important because it develops a potential space, allowing appropriate beacon placement. In fact, creation of an appropriate perirectal weal is the integral step in avoiding deployment of Calypso beacons into the bladder.
6) Using the sagittal orientation on the ultrasound probe, transponders are placed in a triangulated fashion around the vesico-urethral anastamosis with one transponder distally and two proximally, Figure 2.
Care is taken to separate the beacons at least 1 cm apart from one another, in accordance with the manufacturer’s instructions. To date, placement of a foley catheter to help delineate the surrounding anatomy has not been necessary. In fact, we feel that this may, indeed, create ultrasonographic artifact, making placement more difficult. In our experience, needle placement close or into the urethra will elicit a pain response from the patient, requiring adjustment of needle course.
7) Transponders are placed in all patients in an identical location pattern, with one beacon on either lateral aspect of the vesicourethral anastomosis and one in the retrovesical tissue approximately at the level where the seminal vesicles had been.
8) Successful placement is confirmed in all cases by subsequent CT during treatment planning.
9) The endorectal probe is then removed, and the patient is transferred to a modified recovery area.
10) The patient’s vitals signs are monitored, and the patient is observed for presence of rectal bleeding. Prior to being discharged to home, the patient must void, documenting an acceptable post-void residual.
Radiation therapy post-procedure follow up
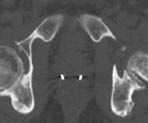
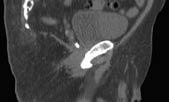
One week after transponder placement, a non-contrast CT scan, Figures 3a and 3b, is obtained under the supervision of the treating radiation oncologist according to the following parameters (FOV = 48 cm; matrix = 512 x 512): from 2 cm above the iliac crest to 2 cm above the femoral heads with 1 cm slice thickness; from 2 cm above the femoral heads to the bottom of the ischial tuberosities using 3 mm slice thickness; and from the bottom of the ischial tuberosities to 12 cm caudal using 1 cm slice thickness. The resultant images are transferred to a treatment planning workstation where a CT-MRI fusion is performed employing chamfer matching and maximization of mutual information techniques. Once the fusion is complete, the critical structures are contoured, including the prostatic fossa, bladder and rectum, as well as the femoral heads, skin and small bowel. The transponder beacons are also identified during this process and their location is registered by the software. An intensity-modulated radiation therapy (IMRT) plan is generated that will cover the planned target volume while limiting the dose to the bladder and rectum. The stored location of the beacons is where the transponders are expected to be found during daily RT treatments, and the Calypso system compares the expected location to the actual location of the transponders prior to the beginning of each treatment session. By convention, a greater than 5 mm intrafraction movement in any direction would result in a cessation of the daily fractionated dose and a realignment of the Calypso system. In order to realign the system, a repeat CT scan must be performed to re-contour the critical structures in relation to the new location of one of the transponders.
Once RT is begun, toxicities are assessed weekly. Upon completion of treatment, patients are seen at 3 and 6 months and every 6 months thereafter with a serum PSA and for symptom reassessment and side effect profile using the AUA-SS and SHIM.
Discussion
We recently published our initial experience with post-prostatectomy Calypso transponder beacon placement technique in two patients receiving adjuvant RT and 15 patients receiving salvage RT.10 No complications were noted in our initial patient cohort. Specifically, during the implantation and throughout the IMRT course, no cases of hematuria, urinary retention, febrile illness, or rectal bleeding occurred. All patients received IMRT, with a median dose of 68 Gy (range 64-68). Treatment was well-tolerated, with no Grade 3 or 4 toxicities. No Grade > 2 enteritis was observed. Genitourinary toxicity was noted in approximately 60% of patients, and consisted of Grade 1 and 2 frequency and dysuria.
For patients who had at least 6 months of follow up after the completion of treatment, all had a PSA value that was undectable (< 0.1 ng/mL). In addition, no changes were noted in the AUA-SS in patients who had completed treatment. The median pre-treatment AUA-SS was 5 and the median post-treatment AUA-SS was 3. Most patients in the cohort suffered from erectile dysfunction and the median pre- and post-treatment SHIM scores were 5.
During treatment, transponder location did not differ significantly from the anticipated location that was calculated during treatment planning. For no patient was a repeat CT scan necessary, signifying that the transponder location was durable and stable. Furthermore, the transponders moved very little during daily treatments.
To our knowledge, our experience with the implantation of electromagnetic transponders into the prostatic bed after radical prostatectomy represents the first series detailing this technique for patients undergoing adjuvant or salvage RT. Since our original report, we have continued to employ this treatment strategy for post-surgical RT with promising oncological results and extremely favorable side-effect profile. Furthermore, treatment planning reconfiguring due to transponder migration has not been encountered to date. Prior to our results, only a single series reported the implantation of gold seed fiducials in patients undergoing RT following RP.9 In this study, Schiffner et al described their experience in 10 patients and found that the use of image-guided target localization was a valuable tool to correct for daily target motion and thereby decrease positioning error.9 The authors noted that the procedure was safe, with no instances of seed migration or toxicities attributable to the implantation. Since this initial report, there has not been any published follow up of this technique. In contrast to other techniques, the benefit of the wireless beacon system is that it allows for daily real-time tracking and monitoring for target localization in order to maximize the amount of radiation that can be delivered to the prostatic bed while minimizing adjacent organ exposure.
Conclusions
The use of electromagnetic transponders for the delivery of salvage or adjuvant radiation therapy allows for daily target positioning correction, offering the opportunity to maximize delivery of radiation to the intended target while minimizing spread to normal adjacent structures. Although this technique is evolving, there appears to be excellent positional stability of the beacons after placement and during treatment. The acute toxicity profile as well as the short-term functional and oncologic outcomes to date have shown great promise. This technique is feasible but does require the Calypso system in order to adopt and implement.